Comprehensive Guide to Stress, Clinical Psychology, and Treatment
This study guide covers the critical intersection of health psychology and clinical psychology. It explores how we process stress, how psychological disorders are classified and diagnosed via the DSM-5, and the various therapeutic modalities used to treat them. This material aligns with the AP Psychology curriculum (often covering topics found in Units 7, 8, and 9).
1. Stress, Coping, and Health Psychology
Health psychology looks at the reciprocal relationship between the mind and the body. The central concept is Stress—not just a stimulus, but a process.
A. Theories of Stress and Appraisal
Stress is definitively described as the process by which we perceive and respond to events, called stressors, that we appraise as threatening or challenging.
1. Hans Selye’s General Adaptation Syndrome (GAS)
Selye discovered that the body’s adaptive response to stress is general—it responds the same way regardless of the specific stressor.
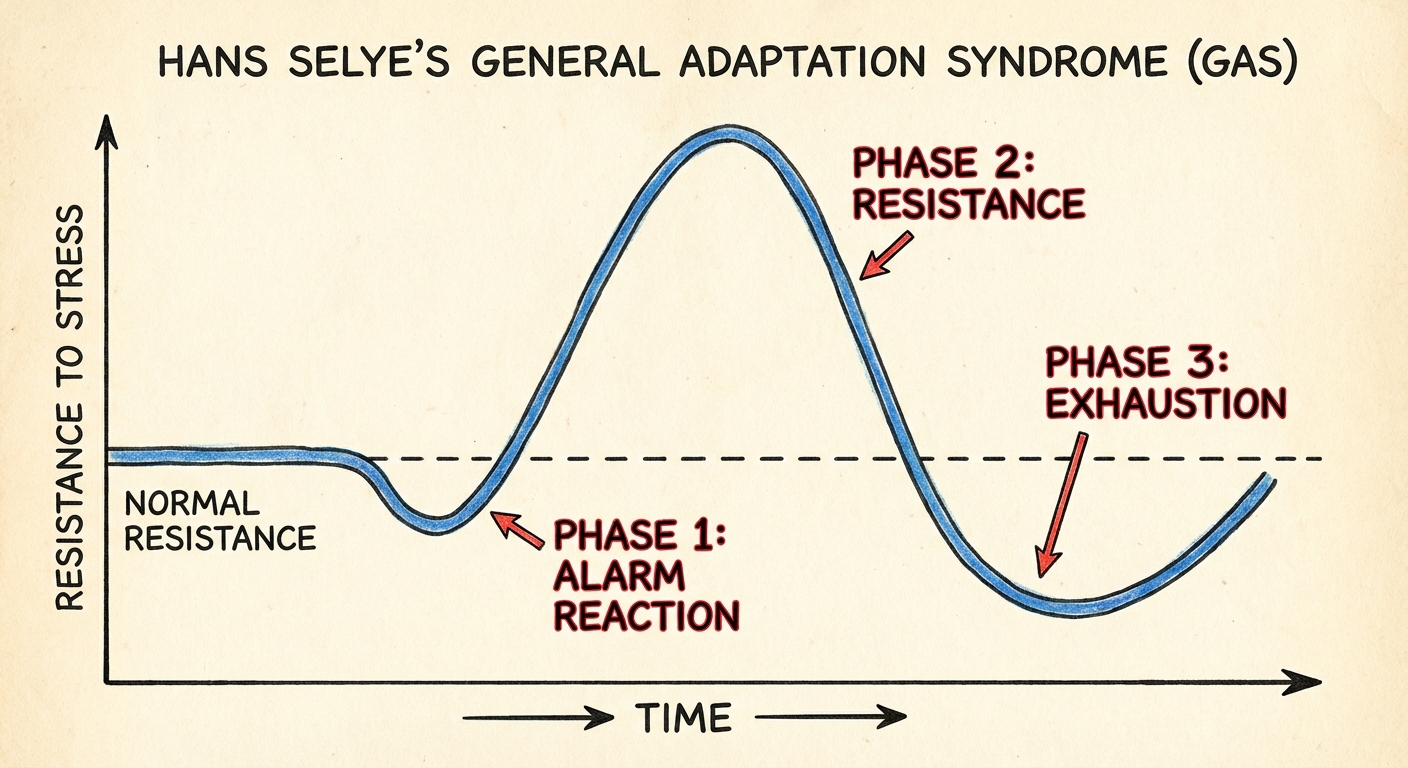
- Phase 1: Alarm Reaction: The "fight-or-flight" response acts as an emergency mobilization. The sympathetic nervous system activiates, heart rate zooms, and blood is diverted to muscles. You may feel faint from shock.
- Phase 2: Resistance: The body remains physiologically ready (high temperature, blood pressure, respiration). Hormones (adrenaline, cortisol) pump into the bloodstream. You can cope with the stressor, but reserves begin to dwindle.
- Phase 3: Exhaustion: If stress is persistent, the body's reserves run out. You become vulnerable to psychosomatic illness (e.g., ulcers, heart disease) or even collapse and death.
2. Lazarus’s Cognitive Appraisal Theory
Stress reflects how we view the event, not the event itself.
- Primary Appraisal: Is this event relevant to me? Is it a threat, a challenge, or benign?
- Secondary Appraisal: Do I have the resources/coping mechanisms to handle this?
- Example: A math test is a threat if you haven't studied (High Stress), but a challenge if you are prepared (Eustress/Positive Stress).
3. Lewin’s Motivational Conflicts
Stress often arises from needing to make choices.
- Approach-Approach: Choosing between two attractive options (e.g., Pizza vs. Tacos). Low stress.
- Avoidance-Avoidance: Choosing between two unattractive options (e.g., Cleaning your room vs. Studying for 3 hours). High stress.
- Approach-Avoidance: One event has both attractive and unattractive features (e.g., A new job pays well but requires a long commute).
- Double Approach-Avoidance: Choosing between two options, each having pros and cons (e.g., Choosing colleges).
B. Stress Personalities & Physiology
- Type A Personality: Competitive, hard-driving, impatient, verbally aggressive, and anger-prone. Key Exam Point: Type A individuals are significantly more prone to Coronary Heart Disease due to the anger/hostility component.
- Type B Personality: Easygoing, relaxed.
- Psychoneuroimmunology: The study of how psychological, neural, and endocrine processes together affect the immune system. Chronic stress releases cortisol, which suppresses the immune system, reducing the release of disease-fighting lymphocytes.
2. Clinical Psychology: Diagnosis and Etiology
Psychological disorders are patterns of thoughts, feelings, or behaviors that are deviant, distressful, and dysfunctional (the 3 D's).
A. The DSM-5-TR
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) is the "bible" of diagnosis.
- Function: It creates a standardized language for clinicians to classify disorders.
- Limitation: It classifies illness by symptoms, not by causes (etiology).
- The Rosenhan Study: Famous study where healthy individuals faked hearing voices to get admitted to asylums. Once admitted, normal behaviors were interpreted as symptoms of their "illness," highlighting the danger of labeling and confirmation bias.
B. The Biopsychosocial Approach
Current psychology rejects the medical model (illness is purely physical) in favor of this holistic model: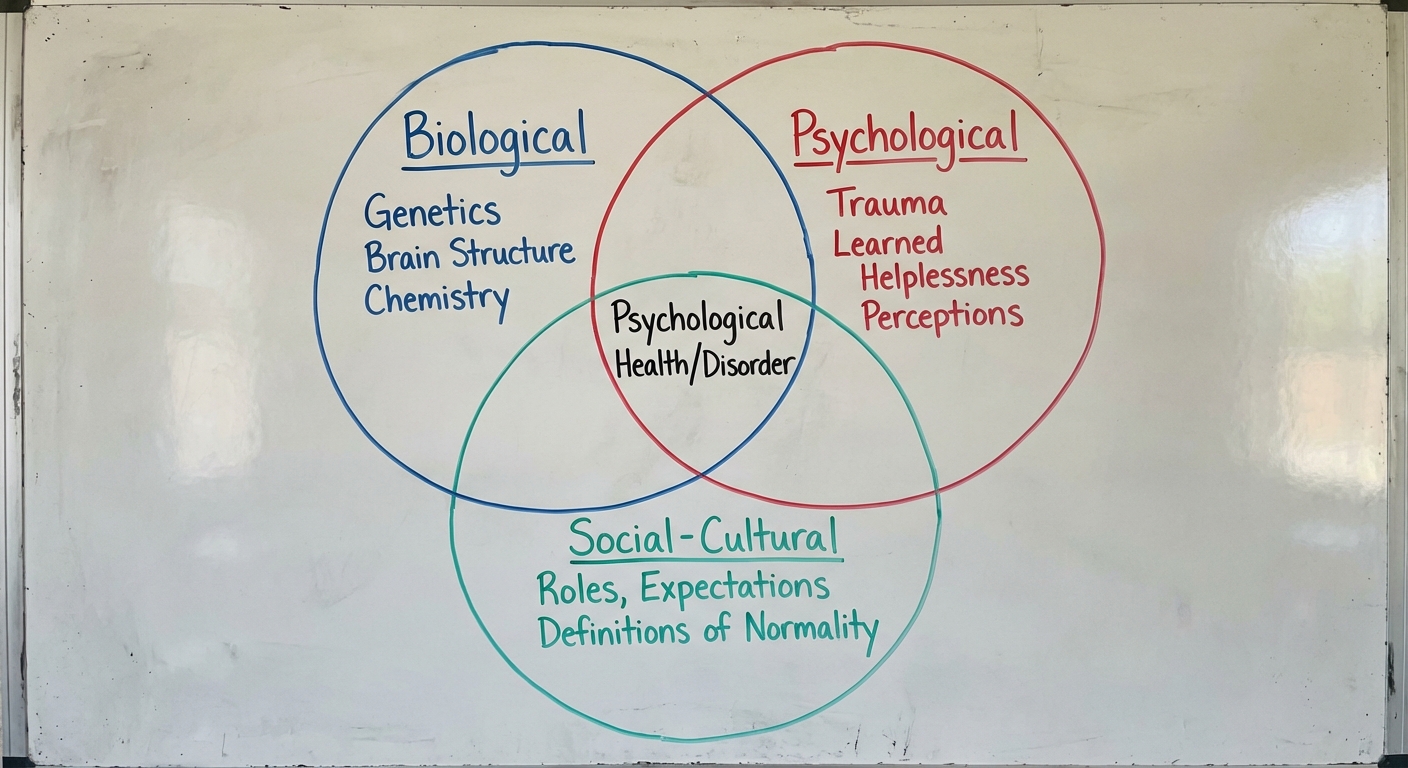
- Biological: Genetics, brain structure, neurotransmitter imbalances.
- Psychological: Stress, trauma, learned helplessness, mood-related perceptions.
- Social-Cultural: Roles, expectations, definitions of "normality."
3. Categories of Psychological Disorders
A. Anxiety Disorders
Characterized by distressing, persistent anxiety or maladaptive behaviors to reduce anxiety.
- Generalized Anxiety Disorder (GAD): Pattern of pathological worry. Unexplainable and continually tense. Autonomic arousal (palpitations, sweating). continually.
- Panic Disorder: Sudden episodes of intense dread (Panic Attacks). Often creates a fear of the fear itself.
- Phobias: Persistent, irrational fear and avoidance of a specific object, activity, or situation (e.g., Agoraphobia: fear of open/crowded spaces).
B. Obsessive-Compulsive & Trauma Disorders
Note: In DSM-5, these are no longer listed under "Anxiety Disorders" but have their own categories.
- OCD (Obsessive-Compulsive Disorder):
- Obsessions: Unwanted, repetitive thoughts (e.g., concern with dirt/germs).
- Compulsions: Repetitive actions typically performed to reduce the anxiety caused by the obsession (e.g., excessive hand washing).
- PTSD (Post-Traumatic Stress Disorder): Characterized by haunting memories, nightmares, social withdrawal, jumpy anxiety, and insomnia lingering for four weeks or more after a traumatic experience.
C. Depressive and Bipolar Disorders (Mood Disorders)
- Major Depressive Disorder (MDD): A state of hopelessness and lethargy lasting two or more weeks. Associated with low Serotonin and Norepinephrine.
- Bipolar Disorder: Alternating between depression and Mania (a hyperactive, wildly optimistic state).
- Bipolar I: Full manic episodes.
- Bipolar II: Hypomanic episodes (less severe) and major depression.
D. Schizophrenia Spectrum
A disconnection from reality (Psychosis). Onset is typically late teens/early 20s.
- Positive Symptoms (Added behaviors): Hallucinations (mostly auditory), Delusions (false beliefs of persecution or grandeur), disorganized speech (word salad).
- Negative Symptoms (Removed behaviors): Flat affect (no emotion), catatonia (motionless), social withdrawal.
- Etiology: Linked to excess Dopamine receptors (Dopamine Hypothesis), enlarged brain ventricles, and prenatal viral infections.
E. Somatic and Dissociative Disorders
- Somatic Symptom Disorder: Symptoms take a somatic (bodily) form without apparent physical cause (e.g., vomiting, dizziness).
- Conversion Disorder: Functional neurological symptom disorder (e.g., unexplained paralysis or blindness).
- Illness Anxiety Disorder: (Formerly Hypochondria) Interpreting normal sensations as symptoms of a dread disease.
- Dissociative Disorders: Conscious awareness becomes separated (dissociated) from previous memories/feelings.
- DID (Dissociative Identity Disorder): Two or more distinct and alternating personalities control a person's behavior. Often linked to severe childhood trauma.
F. Personality Disorders
Inflexible and enduring behavior patterns that impair social functioning. Grouped into three clusters:
- Cluster A (Weird/Eccentric): Schizoid, Paranoid.
- Cluster B (Wild/Dramatic):
- Anti-social PD: Lack of conscience for wrongdoing; aggressive, ruthless (formerly sociopath/psychopath).
- Narcissistic PD: Exaggerated sense of self-importance, need for admiration.
- Borderline PD: Unstable mood, relationships, and self-image.
- Cluster C (Worried/Fearful): Avoidant, Dependent.
4. Treatment and Therapy
A. Psychological Therapies
| Therapy Type | Key Figures | Focus | Key Techniques |
|---|---|---|---|
| Psychoanalysis | Sigmund Freud | Unconscious conflicts from childhood. | Free Association, Dream Analysis, Transference (transferring feelings for parents onto therapist). |
| Humanistic | Carl Rogers, Maslow | Self-fulfillment, self-awareness, present & future (not past). | Client-Centered Therapy, Active Listening, Unconditional Positive Regard. |
| Behavioral | Skinner, Pavlov, Wolpe | Changing unwanted behaviors through learning principles. | Counterconditioning, Systematic Desensitization (for phobias), Aversive Conditioning, Token Economies (Operant conditioning). |
| Cognitive | Aaron Beck | Changing localized negative thought patterns. | Challenging catastrophizing beliefs, Cognitive Triad (Self, World, Future). |
| CBT | Albert Ellis | Combined approach. | REBT (Rational Emotive Behavior Therapy): Vigorously challenging illogical thoughts. |
B. Biomedical Therapies
Treating psychological disorders with medications or medical procedures. This is the realm of Psychiatrists (MDs).
Psychopharmacology (Drug Therapy)
Antipsychotics (Neuroleptics):
- Use: Schizophrenia (Positive symptoms).
- Mechanism: Block Dopamine activity.
- Examples: Thorazine, Haldol, Clozapine.
- Side Effect: Tardive Dyskinesia (involuntary facial muscle movements).
Antianxiety (Anxiolytics):
- Use: Anxiety disorders, panic.
- Mechanism: Depress CNS activity.
- Examples: Xanax, Ativan (Benzodiazepines).
Antidepressants:
- Use: Depression, Anxiety, OCD, PTSD.
- Mechanism: SSRIs (Selective Serotonin Reuptake Inhibitors) block the reuptake of serotonin, leaving more in the synapse.
- Examples: Prozac, Zoloft, Paxil.
Mood Stabilizers:
- Use: Bipolar Disorder.
- Example: Lithium (a simple salt).
Brain Stimulation
- ECT (Electroconvulsive Therapy): Used for severe, treatment-resistant depression. Brief electric current triggers a seizure. Side effect: Short-term memory loss.
- rTMS: Magnetic stimulation (less invasive).
5. Common Mistakes & Pitfalls
- Schizophrenia vs. DID: do NOT confuse these. Schizophrenia is a shattered break from reality (hallucinations). DID is a shattered/split personality. "Schizo" means split mind, but it refers to the split from reality, not multiple personalities.
- Negative Reinforcement vs. Punishment: In disorders, maladaptive behaviors are often maintained by negative reinforcement. Example: Washing hands (behavior) removes anxiety (aversive stimulus). This increases the washing behavior. It is NOT punishment.
- Delusion vs. Hallucination: A Delusion is a false belief (Thinking you are Jesus). A Hallucination is a false sensory experience (Hearing a voice).
- Anti-social Personality Disorder: This does not mean "introverted" or "doesn't like to socialize." In psychology, "anti-social" means against society (criminal, lack of remorse, violation of others' rights).
- Obsession vs. Compulsion: Remember: Obsession = Thought; Compulsion = Action.