AP Psychology: Clinical Treatment & Interventions
Psychotherapy: The Psychological Approach
Psychotherapy refers to an interaction between a trained therapist and someone suffering from psychological difficulties. The goal is to achieve personal growth or overcome symptoms through psychological techniques rather than medical intervention. These therapies generally align with the major perspectives of psychology.
1. Psychoanalysis and Psychodynamic Therapy
Sigmund Freud developed the first strict form of psychotherapy, Psychoanalysis. His central premise was that psychological problems originate from repressed childhood impulses and conflicts.
- Goal: To bring repressed feelings into conscious awareness so the patient can deal with them (insight).
- Techniques:
- Free Association: The patient says whatever comes to mind, no matter how trivial or embarrassing, to bypass the ego's censor.
- Dream Analysis: Interpreting the manifest content (storyline) to find the latent content (hidden meaning).
- Transference: The patient redirects feelings from other relationships (e.g., love or hatred for a parent) onto the therapist.
Psychodynamic Therapy: This is the modern evolution of psychoanalysis. It is shorter, face-to-face (not lying on a couch), and focuses less on the id/sex and more on current relationships and symptom relief, though it still looks for unconscious patterns.
2. Humanistic Therapies
Humanistic therapy, particularly Client-Centered Therapy (developed by Carl Rogers), emphasizes people's inherent potential for self-fulfillment. It focuses on the present and future rather than the past.
- Goal: To help clients grow in self-awareness and self-acceptance (promoting the "ideal self").
- Core Conditions (The Environment):
- Genuineness: The therapist is authentic.
- Unconditional Positive Regard: A caring, nonjudgmental attitude toward the client, accepting them totally.
- Empathy: The therapist reflects the client's feelings.
- Active Listening: A key technique where the therapist echoes, restates, and clarifies what the client says without interpreting it for them.
3. Behavioral Therapies
Behaviorists doubt the healing power of self-awareness. They assume the problem behaviors are the problem and apply learning principles (Classical and Operant Conditioning) to eliminate them.
Classical Conditioning Techniques
Used primarily for phobias and anxiety disorders.
- Counterconditioning: Linking new, positive responses to stimuli that previously triggered unwanted behaviors.
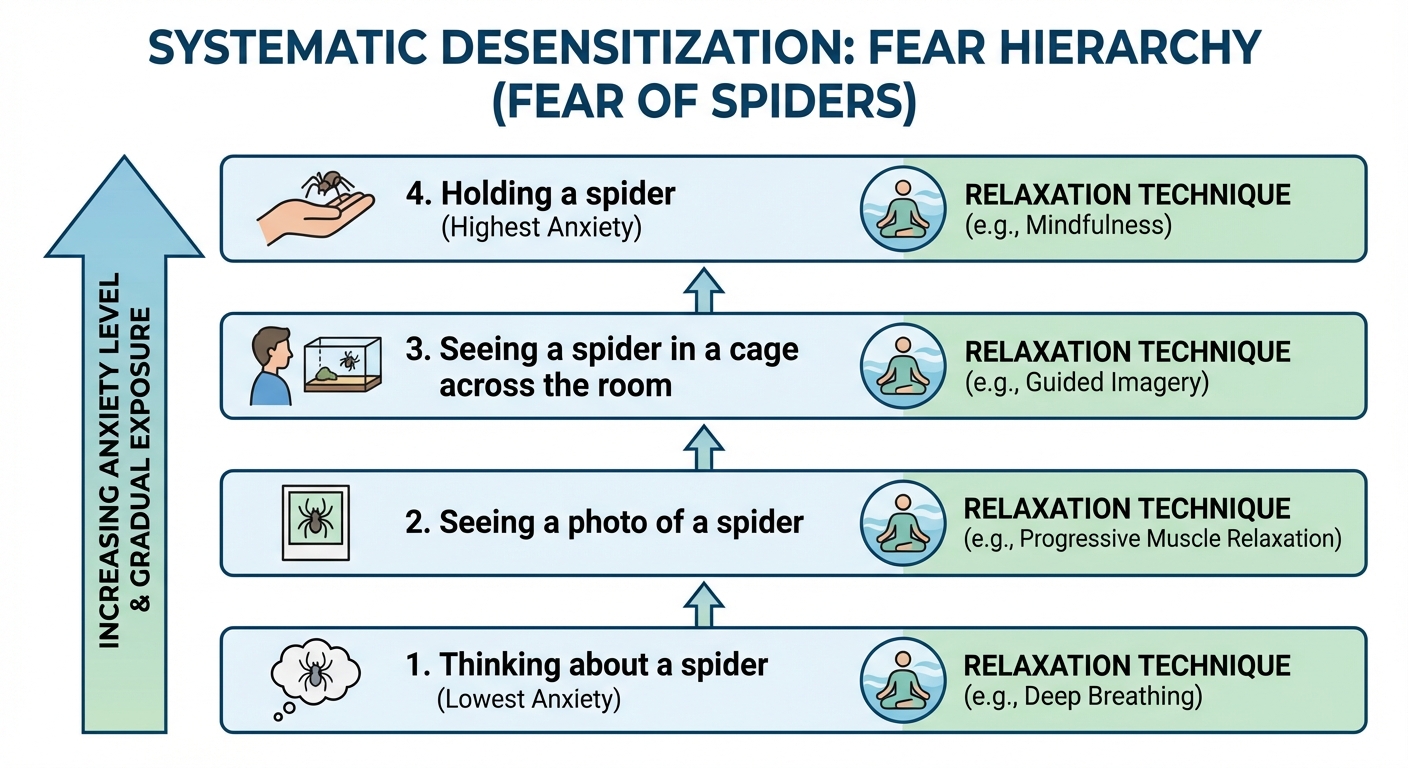
- Exposure Therapy: Treating anxieties by exposing people (in imagination or actual situations) to the things they fear and avoid.
- Systematic Desensitization: A specific type of exposure therapy (associated with Joseph Wolpe). The patient associates a pleasant relaxed state with gradually increasing anxiety-triggering stimuli using a fear hierarchy.
- Aversive Conditioning: Associates an unpleasant state (like nausea) with an unwanted behavior (like drinking alcohol). Effective in the short term, but relapse is common.
Operant Conditioning Techniques
- Behavior Modification: Reinforcing desired behaviors and withholding reinforcement for undesired behaviors.
- Token Economy: An institutional setting (like a school or hospital) where patients exchange a token of some sort—earned for exhibiting the desired behavior—for various privileges or treats.
4. Cognitive and Cognitive-Behavioral Therapies
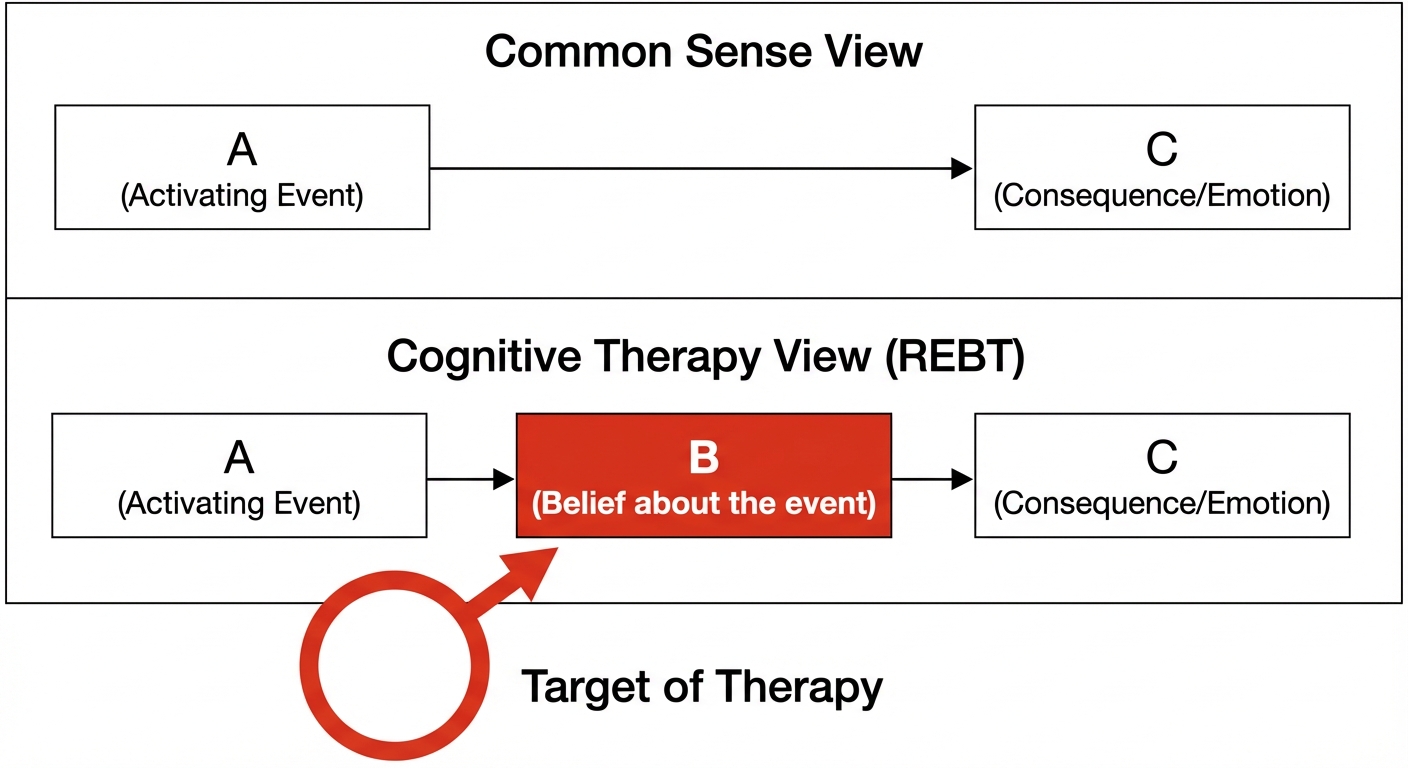
Cognitive therapists teach people new, more adaptive ways of thinking. The assumption is that between the Event and the Response lies the Thought, and the thought creates the emotional reaction.
- Rational-Emotive Behavior Therapy (REBT): Created by Albert Ellis. It is a confrontational therapy that vigorously challenges people's illogical, self-defeating attitudes and assumptions.
- Cognitive Therapy for Depression: Created by Aaron Beck. Gentler than REBT, it uses questioning to help clients reverse "catastrophizing" beliefs about themselves, their situations, and their futures.
Cognitive-Behavioral Therapy (CBT): The most widely practiced integrative therapy today. It aims to alter the way people think (cognitive) and the way they act (behavioral). It is highly effective for anxiety and mood disorders.
Biomedical Therapies
Biomedical therapy physically changes the brain's functioning. This is the implementation of the Medical Model.
Psychopharmacology (Drug Therapies)
This is the study of the effects of drugs on mind and behavior. Standardized testing (double-blind studies) is crucial here.
| Drug Class | Primary Use | Mechanism of Action | Examples | Potential Side Effects |
|---|---|---|---|---|
| Antipsychotics | Schizophrenia (Positive symptoms like hallucinations) | Antagonist: Blocks Dopamine receptors | Thorazine, Haldol, Risperdal | Tardive Dyskinesia (involuntary facial muscle movements) |
| Antianxiety | Anxiety Disorders, PTSD, OCD | Depresses central nervous system activity (increases GABA) | Xanax, Ativan | Dependence/Addiction, drowsiness |
| Antidepressants | Depression, Anxiety Disorders | Agonist: Increases Serotonin or Norepinephrine (SSRIs and SNRIs) | Prozac, Zoloft, Paxil | Dry mouth, weight gain, sexual dysfunction |
| Mood Stabilizers | Bipolar Disorder | Stabilizes mania and depression episodes | Lithium (simple salt), Depakote | Thirst, tremors |
Brain Stimulation
- Electroconvulsive Therapy (ECT): A biomedical therapy for severely depressed patients in which a brief electric current is sent through the brain of an anesthetized patient. It is effective but controversial due to memory loss risks.
- Repetitive Transcranial Magnetic Stimulation (rTMS): The application of repeated pulses of magnetic energy to the brain; used to stimulate or suppress brain activity.
Psychosurgery
Surgery that removes or destroys brain tissue in an effort to change behavior. This is the most drastic and least used intervention.
- Lobotomy: Historically used to disconnect emotion from thought by cutting nerves connecting the frontal lobes to the emotion-controlling centers. Rarely performed now.
Evaluating Treatment Effectiveness
How do we know if therapy works? We cannot rely solely on client testimonials because people often enter therapy in crisis and might improve naturally over time.
Challenges to Evaluation
- The Placebo Effect: The power of belief in a treatment. If you think the treatment will work, your mood may improve regardless of the therapeutic technique.
- Regression to the Mean: The tendency for extreme or unusual scores (or emotions) to fall back (regress) toward their average. If you are at rock bottom, you will likely improve somewhat regardless of what you do.
The Verdict: Evidence-Based Practice
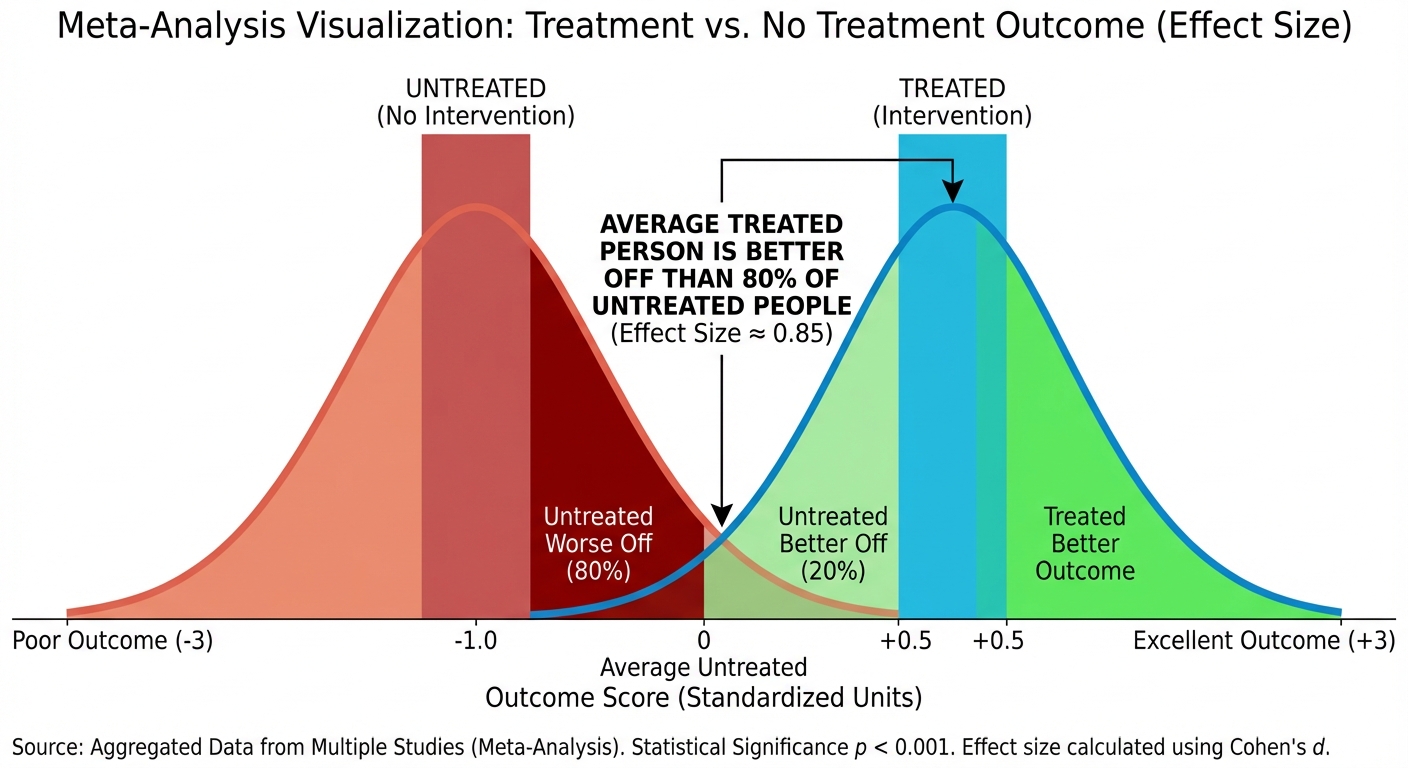
Meta-analysis (a procedure for statistically combining the results of many different research studies) shows that:
- Those receiving therapy improve faster and with less risk of relapse than those who do not.
- No single type of therapy is universally "best," but some are better for specific disorders (e.g., Behavioral used for phobias; Cognitive used for depression).
The Therapeutic Alliance: The most important common factor in successful therapy is the emotional bond between therapist and client—a relationship built on mutual trust and understanding.
Common Mistakes & Pitfalls
- Systematic Desensitization vs. Flooding: Students confuse these. Systematic is gradual (step-by-step hierarchy). Flooding is immediate exposure to the worst-case scenario. Both are exposure therapies, but the pacing differs.
- REBT vs. Cognitive Therapy: Both are cognitive, but remember the style. Albert Ellis (REBT) is confrontational (arguing against the irrational thought). Aaron Beck is gentle (asking questions to lead the client to authorized realization).
- Antipsychotic Side Effects: Do not forget Tardive Dyskinesia. It is a specific, high-frequency test question regarding long-term use of dopamine blockers.
- Negative Reinforcement vs. Punishment in Therapy: In behavior modification, remember that Negative Reinforcement strengthens a behavior by removing something bad. Punishment stops a behavior. Therapy often prefers reinforcement over punishment.
- Dopamine vs. Serotonin: Don't mix them up. Dopamine excess = Schizophrenia (treat with Antipsychotics). Serotonin deficit = Depression (treat with SSRIs).