Clinical Psychology: Comprehensive Guide to Abnormal Behavior
Clinical Psychology: Comprehensive Guide to Abnormal Behavior
Introduction to Psychological Disorders
Understanding psychological disorders requires moving beyond lay terms like "crazy" or "insane." In psychology, we use rigorous criteria to distinguish between normal variations in human behavior and clinically significant disorders.
Defining Abnormality
To classify a set of behaviors as a Psychological Disorder, psychologists generally look for the "Maladaptive" criteria, often summarized as the Three D's (sometimes four):
- Distress: The behavior causes significant personal anguish or discomfort.
- Dysfunction: The behavior interferes with daily functioning (work, relationships, hygiene). This is often considered the key boundary between a quirk and a disorder.
- Deviance: The behavior strays significantly from societal norms (though this varies by culture).
- (Optional 4th D) Danger: Does the behavior pose a threat to the self or others?
Note: "Insanity" is a legal term, not a psychological diagnosis. It is used in court to determine if a defendant can be held criminally liable for their actions.
The Biopsychosocial Approach
Modern clinical psychology rejects the idea that disorders have a single cause. Instead, we use the Biopsychosocial Model to understand etiology (cause).
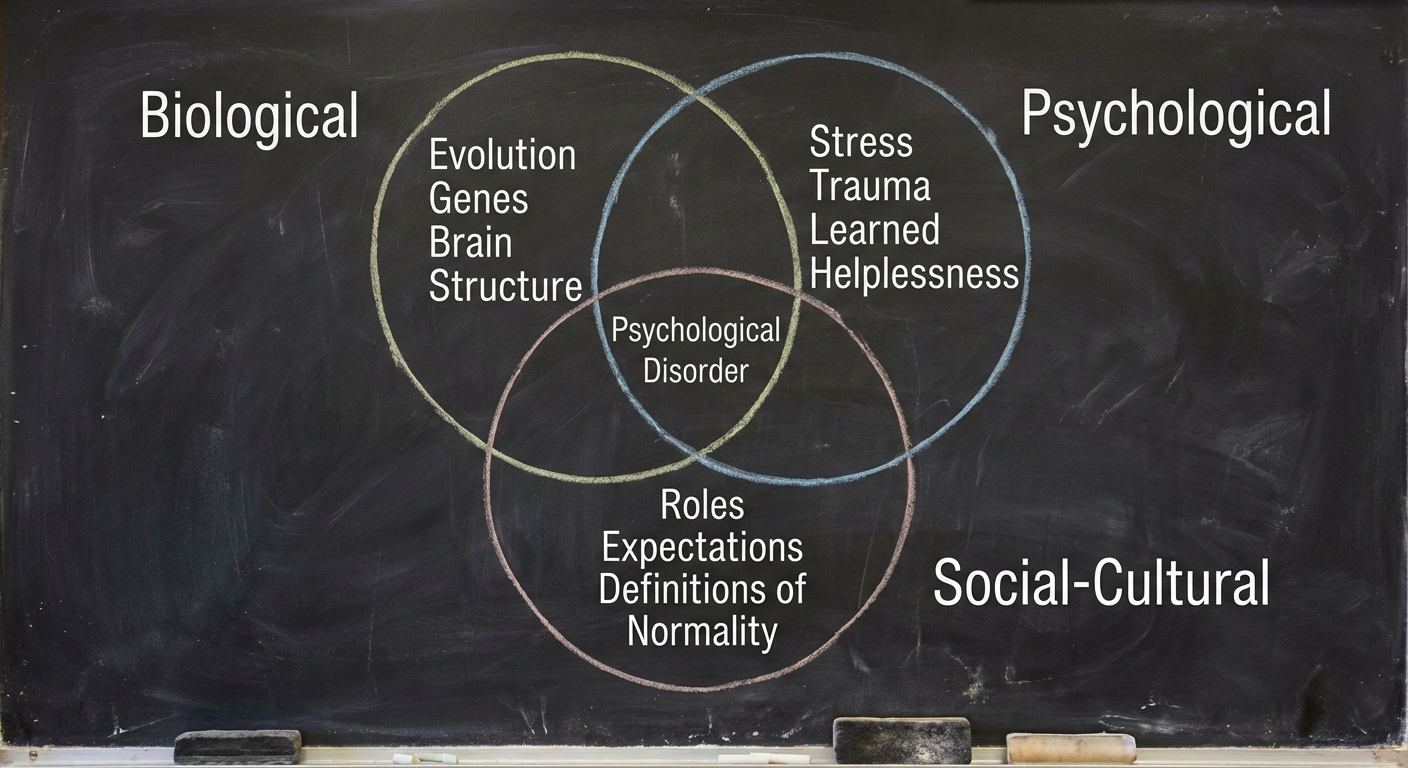
- Biological: Genetic predisposition, brain structure, and neurochemistry (e.g., serotonin levels).
- Psychological: stress, trauma, learned helplessness, and mood-related perceptions.
- Social-Cultural: Roles, expectations, cultural definitions of normality, and definitions of disorder.
The DSM-5-TR
Psychologists use the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision (DSM-5-TR) to classify disorders.
- Purpose: It contains diagnostic criteria and codes to standardize diagnoses.
- Important Limitation: It classifies disorders (describes symptoms) but does not explain their causes (etiology) or outline treatments.
The Rosenhan Study (1973)
A classic study highlighting the danger of labeling. David Rosenhan and colleagues faked hallucinations to get admitted to psychiatric hospitals. Once inside, they acted normally, but staff interpreted their normal behavior as symptoms of their diagnosis. This proved that diagnostic labels can create bias and stigma.
Anxiety, Obsessive-Compulsive, and Trauma-Related Disorders
In the DSM-5, these are three distinct categories, but they share the underlying theme of excessive fear or worry.
Anxiety Disorders
Characterized by distressing, persistent anxiety or maladaptive behaviors that reduce anxiety.
- Generalized Anxiety Disorder (GAD): A person is unexplainably and continually tense and uneasy. It is often called "free-floating anxiety" because the person cannot identify the cause.
- Symptoms: Autonomic arousal (sweating, trembling), worry, inability to concentrate.
- Panic Disorder: Marked by unpredictable, minutes-long episodes of intense dread known as Panic Attacks.
- Symptoms: Chest pain, choking, terror. Often leads to fear of the next attack.
- Phobias: Persistent, irrational fear and avoidance of a specific object or situation.
- Specific Phobias: Spiders (arachnophobia), heights (acrophobia), etc.
- Social Anxiety Disorder: Intense fear of social situations, leading to avoidance of scrutiny.
- Agoraphobia: Fear of entering open or crowded places where escape might be difficult (often develops after Panic Disorder).
Obsessive-Compulsive Disorder (OCD)
OCD is a cycle of unwanted repetitive thoughts and actions.
- Obsessions: Intrusive, repetitive thoughts (e.g., "My hands are covered in deadly germs").
- Compulsions: Repetitive behaviors performed to reduce the anxiety caused by the obsession (e.g., washing hands exactly 20 times).
Key Concept: The behavior is compulsive only if it disrupts life and is done strictly to relieve the anxiety of the obsession.
Post-Traumatic Stress Disorder (PTSD)
Develops after exposure to a traumatic event (war, assault, accident).
- Symptoms: Haunting memories (flashbacks), nightmares, social withdrawal, jumpy anxiety, and distinct insomnia lasting four weeks or more.
- Post-Traumatic Growth: The positive psychological changes as a result of struggling with extremely challenging circumstances.
Depressive and Bipolar Disorders
These are disorders of mood (affect).
Major Depressive Disorder (MDD)
Often called the "common cold" of mental health due to its prevalence. To be diagnosed, a person must experience symptoms for at least two weeks.
- Symptoms: Depressed mood, diminished interest in activities (anhedonia), weight/appetite changes, insomnia/hypersomnia, fatigue, feelings of worthlessness.
- Biological Perspective: Low levels of Serotonin and Norepinephrine; reduced activity in the left frontal lobe.
- Social-Cognitive Perspective:
- Learned Helplessness: The passive resignation learned when unable to avoid repeated aversive events.
- Rumination: Compulsive fretting; overthinking about our problems and their causes.
- Explanatory Style: Depressed individuals often explain bad events as Stable ("It will last forever"), Global ("It will affect everything I do"), and Internal ("It's all my fault").
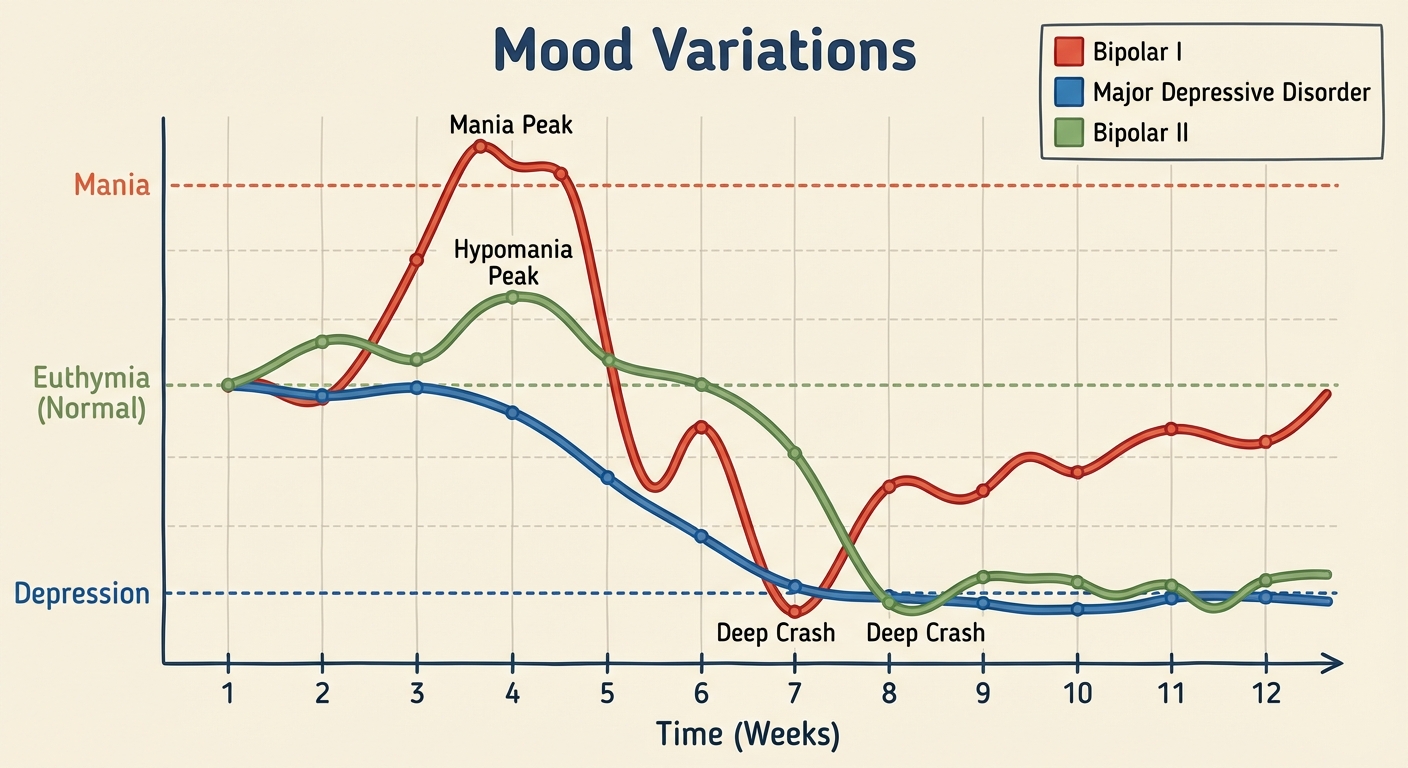
Bipolar Disorder
Characterized by alternating between depression and Mania.
- Mania: A hyperactive, wildly optimistic state. Symptoms include rapid speech (pressured speech), grandiosity, little need for sleep, and risky behavior (spending sprees, unsafe sex).
- Bipolar I: Full manic episodes followed by depressive episodes.
- Bipolar II: Hypomanic (less severe mania) episodes and depressive episodes.
Schizophrenia and Dissociative Disorders
Schizophrenia Spectrum
Schizophrenia is a Psychotic Disorder characterized by a break from reality (psychosis). The onset is typically late adolescence/early adulthood.
Symptoms
We categorize symptoms into "Positive" (added) and "Negative" (subtracted).
| Type | Definition | Examples |
|---|---|---|
| Positive Symptoms | Presence of inappropriate behaviors (things that are there but shouldn't be). | Hallucinations (false sensory experiences, mostly auditory), Delusions (false beliefs, e.g., persecution or grandeur), Disorganized speech ("word salad"). |
| Negative Symptoms | Absence of appropriate behaviors (things that should be there but aren't). | Flat Affect (show no emotion), Catatonia (motionlessness for hours), social withdrawal. |
Etiology of Schizophrenia
- Dopamine Hypothesis: High levels of dopamine (or over-sensitive receptors) are linked to positive symptoms (hallucinations).
- Brain Structure: Enlarged fluid-filled ventricles; shrinkage of cerebral tissue.
- Prenatal Factors: Viral infections (like the flu) during the second trimester of pregnancy.
Dissociative Disorders
These involve a disruption in conscious awareness, memory, or identity. They are rare and controversial.
- Dissociative Identity Disorder (DID): Formerly multiple personality disorder. A person exhibits two or more distinct and alternating personalities.
- Controversy: Critics argue DID may be created by therapists asking leading questions or acts as a role-playing response to trauma.
- Dissociative Amnesia: Inability to recall important personal information, usually of a traumatic nature.
- Dissociative Fugue: A sudden loss of memory combined with an unexpected travel away from home.
Personality and Neurodevelopmental Disorders
Personality Disorders
Inflexible and enduring behavior patterns that impair social functioning. These are grouped into three clusters.
Cluster B (Dramatic/Impulsive) - The most frequently tested:
- Antisocial Personality Disorder (ASPD): Usually a male who displays a lack of conscience for wrongdoing, even toward friends and family. May be aggressive and ruthless. Historically called a sociopath or psychopath.
- Biological marker: Reduced activity in the frontal lobes (impulse control) and lower levels of autonomic arousal (low stress hormones).
- Narcissistic Personality Disorder: Exaggerated sense of self-importance, need for admiration, and lack of empathy.
- Borderline Personality Disorder (BPD): Unstable mood, behavior, and relationships; fear of abandonment.
Neurodevelopmental Disorders
Diagnosed in childhood, these involve central nervous system abnormalities.
- Autism Spectrum Disorder (ASD): Deficiencies in communication and social interaction; rigidly fixated interests and repetitive behaviors.
- Attention-Deficit/Hyperactivity Disorder (ADHD): Extreme inattention, hyperactivity, and impulsivity.
Somatic Symptom Disorders
Disorders taking a bodily (somatic) form without an apparent physical cause.
- Somatic Symptom Disorder: A person has physical symptoms (e.g., nausea, dizziness, pain) coupled with abnormal thoughts, feelings, and behaviors about the symptoms.
- Conversion Disorder: A person experiences very specific physical symptoms (blindness, paralysis) with no physiological basis. Often related to anxiety being "converted" into a physical symptom.
- Illness Anxiety Disorder: (Formerly Hypochondriasis). A person interprets normal physical sensations (a headache) as symptoms of a dreaded disease (brain tumor).
Common Mistakes & Pitfalls
Only 4 to Avoid
- Schizophrenia vs. DID: This is the #1 mistake. Schizophrenia is NOT "split personality." It is a "split mind" referring to a break from reality (psychosis). DID is the presence of multiple personalities.
- Anti-social vs. Introverted: "Antisocial" in psychology does not mean you don't like parties (that's asocial or introverted). Antisocial Personality Disorder means you are against society (criminal, manipulative, lack of remorse).
- Obsession vs. Compulsion: Remember: Obsession is occurring in the brain (thought); Compulsion is the action (behavior). You obsess over germs, so you feel compelled to wash your hands.
- Hallucination vs. Delusion:
- Hallucination = Hearing/Seeing things not there (Sensory).
- Delusion = Disbelief/False idea (Cognitive). If I think I am Jesus, that is a delusion. If I see Jesus in my toast, that is a hallucination.